NORMAL & SINUS RHYTHMS
NORMAL
Normal Sinus Rhythm (NSR)
Rate: 60–100 bpm

Regular P wave before every QRS
PR interval 0.12–0.20s
QRS <0.12s (narrow)
Regular R-R intervals
SINUS
Sinus Bradycardia
Rate: <60 bpm

All features of NSR but rate <60
Prolonged R-R intervals
Normal P, QRS, T morphology
SINUS
Sinus Tachycardia
Rate: 100–150 bpm

All features of NSR but rate >100
P waves may be buried in T waves at fast rates
Regular rhythm
ATRIAL RHYTHMS
ATRIAL
Rapid Atrial Fibrillation (A-Fib)
Atrial: 350–600 bpm · Ventricular: variable

Irregularly irregular — no two R-R intervals equal
No identifiable P waves — chaotic baseline
Narrow QRS (usually)
ATRIAL
Atrial Flutter
Atrial: 250–350 bpm · Ventricular: 75–150 bpm

Sawtooth "flutter waves" — classic pattern
Regular or regularly irregular ventricular rate
2:1, 3:1, or 4:1 conduction ratio
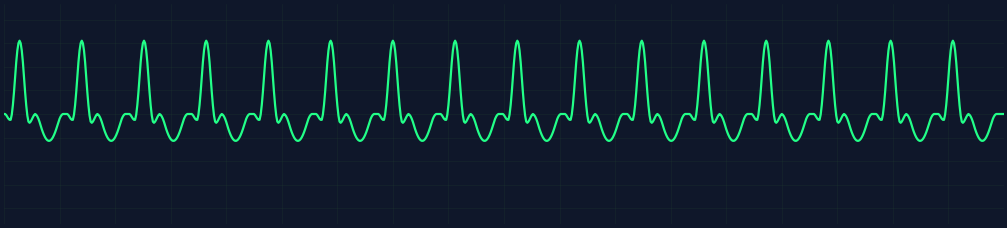
SVT
Supraventricular Tachycardia (SVT)
Rate: 150–250 bpm

Rapid, regular, narrow-complex tachycardia
P waves hidden within or after QRS
Abrupt onset and termination
HEART BLOCKS
1° BLOCK
First-Degree AV Block
Rate: Normal · PR >0.20s

PR interval consistently >0.20s (one big box)
Every P wave conducts — no dropped beats
Regular rhythm, normal QRS
2° TYPE I
Second-Degree Block — Wenckebach
Progressive PR lengthening → dropped QRS

PR interval gets longer with each beat
Eventually a QRS is dropped — then resets
"Longer, longer, longer, drop — then you've got a Wenckebach"
2° TYPE II
Second-Degree Block — Mobitz II
Sudden dropped QRS, no PR change

PR interval CONSTANT — then suddenly drops a QRS
More dangerous than Type I — can progress to 3°
Infranodal block — wide QRS common
3° BLOCK
Third-Degree (Complete) AV Block
Atrial: 60–100 · Ventricular: 20–40 bpm

P waves and QRS have NO relationship — complete dissociation
Both rhythms regular but independent
Ventricular escape rhythm — wide, slow QRS
VENTRICULAR RHYTHMS — HIGH PRIORITY
V-TACH
Ventricular Tachycardia (V-Tach)
Rate: 100–250 bpm
Wide, bizarre QRS complexes (>0.12s)
Regular, rapid — monomorphic
No P waves or dissociated P waves
LETHAL
Fine Ventricular Fibrillation (Fine V-Fib)
No organized rate — low-amplitude chaotic
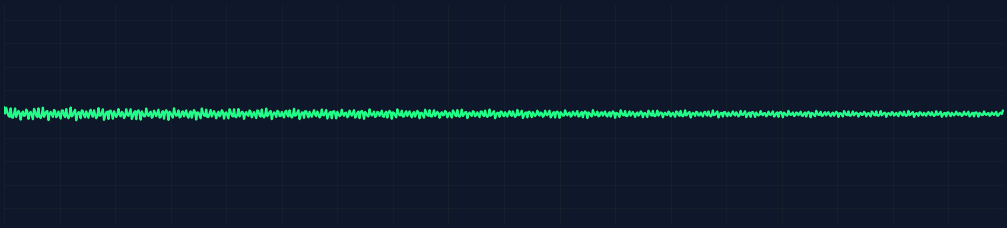
Completely chaotic — no P, QRS, or T
Low amplitude (<3mm) — tight, fuzzy baseline
Prolonged arrest — depleted myocardial energy
PULSELESS — lower defibrillation success rate
LETHAL
Coarse Ventricular Fibrillation (Coarse V-Fib)
No organized rate — high-amplitude chaotic
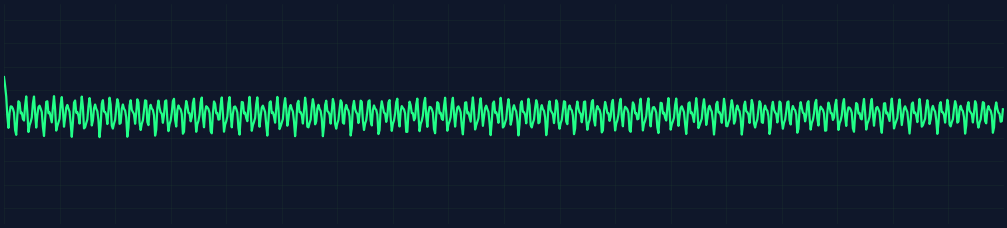
Completely chaotic — no P, QRS, or T
High amplitude (>3mm) — large disorganized deflections
Recent onset — viable myocardium still present
PULSELESS — better defibrillation response than fine VFib
POLYMORPHIC
Torsades de Pointes
Rate: 150–250 bpm · Twisting QRS axis

QRS complexes twist around baseline — "spindle" pattern
Caused by prolonged QT interval
Associated with hypomagnesemia, antiarrhythmics